Neovascularization in Ocular Inflammation
Not all vessels heal—some steal vision
Neovascularization, the pathological formation of new blood vessels, is a fundamental biological response to tissue injury, ischaemia, inflammation, and tumour growth. While physiologically essential for healing, uncontrolled neovascularization in the eye leads to profound and often irreversible visual loss. In the context of uveitis and intraocular inflammation, this process presents a unique clinical challenge: it may arise without the hallmark retinal ischaemia seen in vascular diseases, preferentially targets the optic disc over the peripheral retina, can involve the iris or the vitreous base, and often responds to immunosuppression rather than anti-vascular therapy alone.
Vascular growth is mediated through three interrelated processes: angiogenesis, arteriogenesis, and vasculogenesis, which are functionally inseparable. Capillary formation (angiogenesis) without simultaneous arteriogenesis to supply those capillaries is physiologically futile.
|
Process |
Definition |
|
Angiogenesis |
Formation of new capillaries by sprouting from existing vessels, predominantly from postcapillary venules. The principal mechanism in inflammatory eye disease. |
|
Arteriogenesis |
Remodelling of pre-existing arterioles and collaterals into muscular arteries, and/or de novo formation of vessels with a tunica media. Ensures adequate supply to newly formed capillary beds. |
|
Vasculogenesis |
Formation of entirely new vessels from multipotent endothelial stem cells. Primarily relevant during embryogenesis but may contribute in severe inflammation. |
Vascular Growth Factors
Vascular endothelial growth factor (VEGF) and fibroblast growth factor (FGF) are the principal angiogenic mediators. VEGF-A — the isoform most relevant to angiogenesis, exists in five forms (121, 145, 165, 189, and 206 amino acids). VEGF-C primarily promotes lymphangiogenesis. FGF binds receptors on endothelial cells and fibroblasts, while VEGF receptors are predominantly endothelial. Both stimulate endothelial proliferation and migration, promoting neovascularization in ischaemic and — critically — non-ischaemic inflammatory settings.
Vinores et al. demonstrated upregulation of VEGF not only in ischaemic retinopathies but also in retinal neurons and retinal pigment epithelium in non-ischaemic inflammatory disease, including experimental autoimmune uveoretinitis — with increased immunoreactivity in the ganglion cell layer, inner plexiform layer, and inner nuclear layer. This establishes a direct inflammatory route to VEGF overexpression, independent of ischaemia
Angiogenesis, arteriogenesis and vasculogenesis are functionally coupled, isolated capillary formation without arterial supply is physiologically meaningless.
VEGF is upregulated in ocular inflammation independent of ischaemia, through direct stimulation of retinal ganglion cells, inner plexiform layer, and RPE (Vinores et al.).
TNF-alpha has a bimodal role in angiogenesis: low doses may be pro-angiogenic; high doses inhibitory,a mechanism with direct relevance to JIA-related NVD and anti-TNF therapy.
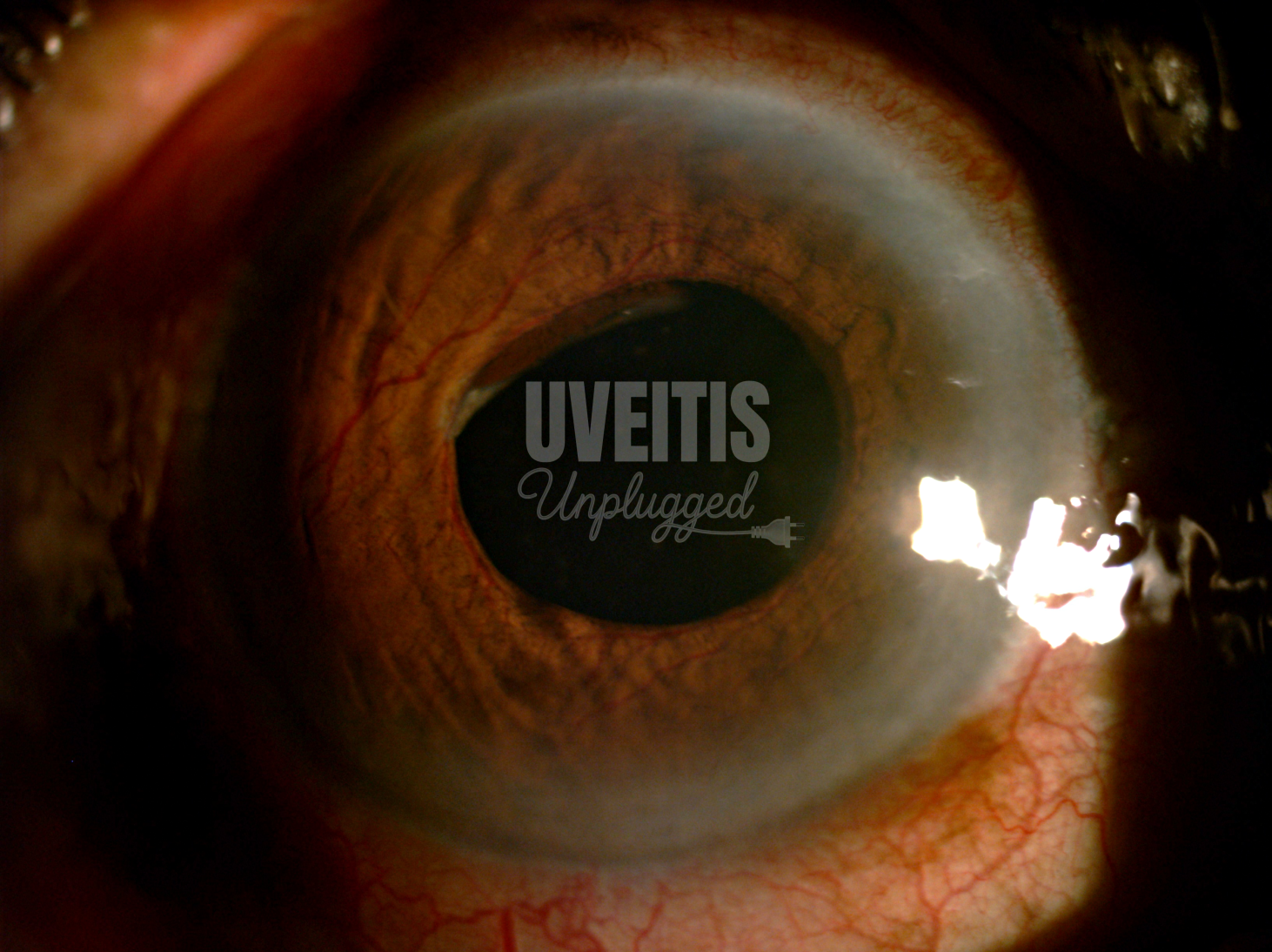
Neovascularization of the Iris (NVI)
Historically termed rubeosis iridis by Salus (1928), neovascularization of the iris (NVI) — the preferred term (Wand) — describes new vessel formation on the anterior iris surface and in the chamber angle. Vessels originate from pre-existing iris capillary beds near the iris root and pupillary margin, forming fine anterior tufts. Unlike normal iris vasculature, these vessels leak fluorescein on angiography. They may remain quiescent for years but often enlarge, with accompanying fibrovascular proliferation causing synechial angle closure and secondary neovascular glaucoma (NVG) — a condition that responds poorly to conventional therapy.
- Early NVI appears as fine vessel tufts at the pupillary margin or angle — requires careful slit-lamp biomicroscopy and gonioscopy for detection.
- Fluorescein leakage distinguishes neovascular from normal iris vessels on angiography.
- Fibrovascular proliferation causes progressive synechial angle closure, leading to NVG refractory to medical treatment.
- Treatment of the underlying inflammatory cause is the cornerstone of management.
- UGH Syndrome (Uveitis-Glaucoma-Hyphaema): originally described by Ellingson (1977) from excessive IOL movement (small/dislocated lens, iris-clipped IOLs, rigid haptics). Now rare with modern posterior chamber IOL designs.
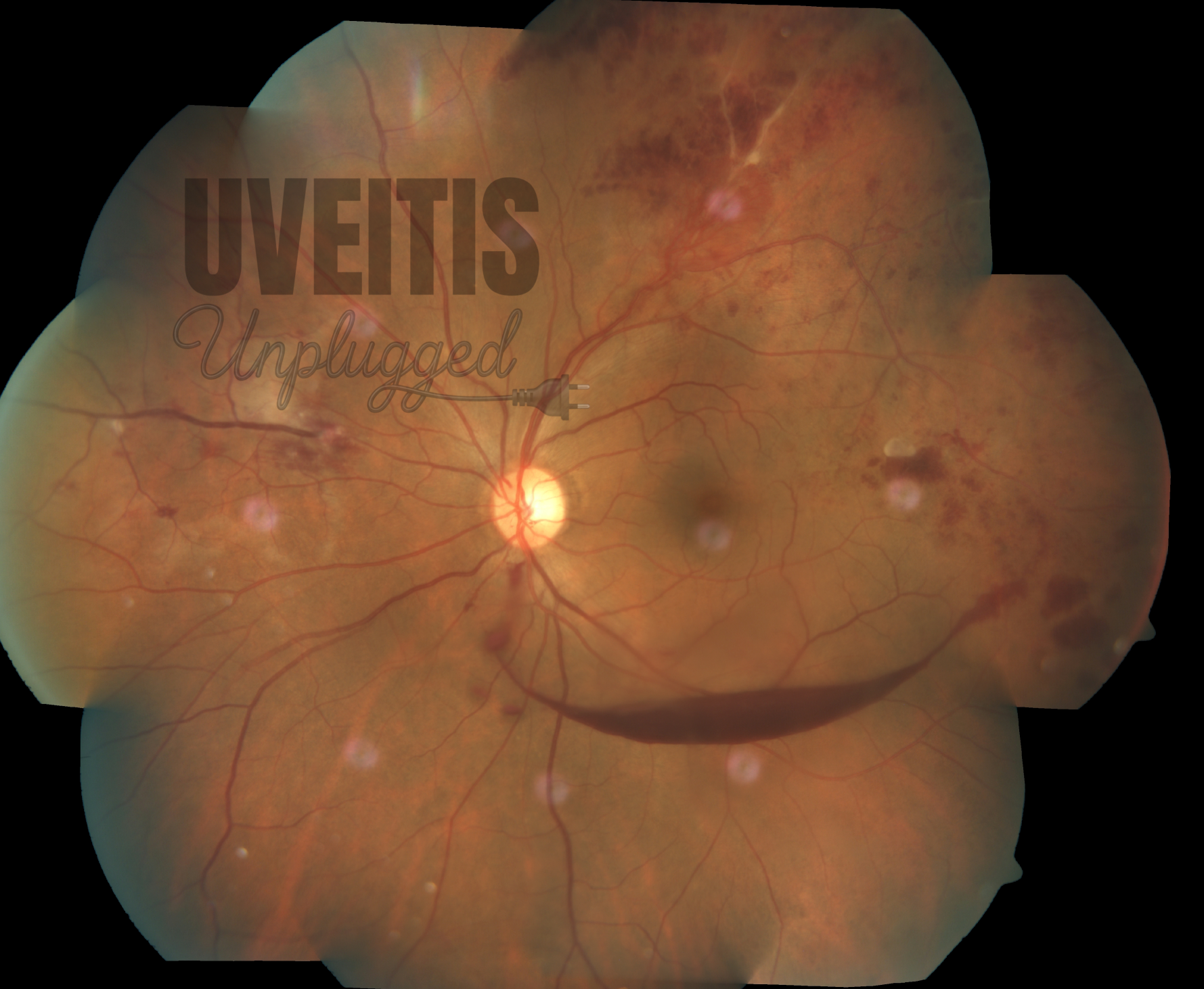
Neovascularization of the Disc (NVD) in Inflammation
Inflammatory NVD is defined by disc neovascularization in the absence of angiographic evidence of extensive retinal capillary non-perfusion. Shorb et al. first described this entity in 1976, reporting five eyes with NVD and chronic uveitis in whom fluorescein angiography excluded retinal ischaemia. This has since been confirmed in multiple case series and reports across diverse uveitic conditions.
Why Does Inflammation Preferentially Target the Optic Disc?
Three complementary mechanisms explain the predilection of inflammatory neovascularization for the optic disc over the peripheral retina:
(i) Vitreopapillary pathway: vasoproliferative factors — principally VEGF — produced by inflamed retinal tissue drain preferentially through this route, resulting in concentrated exposure at the disc margin (Henkind).
(ii) Ciliary circulation involvement: the optic nerve head receives dual vascular supply from the retinal and posterior ciliary circulations, both susceptible to uveitis-mediated vasculopathy (Asdourian et al.).
(iii) Internal limiting membrane differences: the ILM is structurally thinner or absent at the optic disc, offering less mechanical resistance to outward vessel growth (Foos).
Uveitic Conditions Associated with Inflammatory NVD
Inflammatory NVD has been documented in a broad range of conditions — many without demonstrable retinal ischaemia on fluorescein angiography: sarcoidosis, Behcet's disease, JIA-related uveitis, intermediate uveitis, Vogt-Koyanagi-Harada disease, cytomegalovirus retinitis, toxoplasmosis, tubercular serpiginous-like choroiditis (TB-SLC), serpiginous choroiditis, acute retinal necrosis, syphilis, and pars planitis.
In neurosarcoidosis, a sarcoid granuloma may compress the optic nerve and its vasculature, producing retinal circulatory occlusion with widespread ischaemia, elevated aqueous VEGF, and NVG (Vereecken et al., Brown et al.). Importantly, angiogenic cytokines including VEGF are transcriptionally upregulated in sarcoidosis independent of ischaemia (Mikami et al.).
In TB-SLC, extensive confluent choroidal lesions — causing widespread outer retinal atrophy demonstrable on enhanced depth imaging OCT , trigger VEGF upregulation even without angiographic ischaemia, rendering the NVD refractory to corticosteroids (Bansal et al.).
Clinical Pearls: Inflammatory NVD
- Always perform fluorescein angiography in NVD — the absence of retinal capillary non-perfusion defines inflammatory (non-ischaemic) NVD and changes management.
- The optic disc is preferentially targeted in uveitis-related neovascularization because of the vitreopapillary drainage pathway, ciliary circulation involvement, and absent ILM at the disc.
- Behcet's disease: apparent clinical remission can be misleading — monitor for NVD during the post-attack period, especially when the retina remains viable.
- JIA-related NVD: can occur in children as young as 4 years without ischaemia; periocular or systemic corticosteroids usually produce prompt regression.
- TB-SLC: NVD may be steroid-resistant due to VEGF upregulation from widespread outer retinal damage — anti-VEGF adjuncts are important.
- Up to 30% of inflammatory NVD cases remain resistant to immunosuppression, with attendant risk of permanent visual loss.
- Partial NVD regression typically occurs within 2-6 weeks of corticosteroid initiation; complete resolution may take 2-42 months; recurrences are documented (Sanislo et al.).
- Most affected patients are relatively young, with a slight female predominance reported in earlier series.
Treatment Approach: Inflammatory NVD
Step 1 — Investigate: Fluorescein angiography to confirm non-ischaemic NVD; screen for systemic associations (chest X-ray, ACE, IGRA/Mantoux, syphilis serology, ANA).
Step 2 — Treat the cause: Systemic corticosteroids and/or disease-specific immunosuppression (antitubercular, antiviral, biologic agents as indicated).
Step 3 — Adjunct anti-VEGF: Add intravitreal anti-VEGF (e.g., ranibizumab) for steroid-resistant, recurrent, or anatomically threatening NVD.
Step 4 — Anti-TNF consideration: In JIA-related NVD unresponsive to corticosteroids, anti-TNF biologic therapy is a rational option.
Step 5 — Long-term follow-up: Resolution may take many months; monitor closely for recurrence even after apparent regression.
Neovascularization Elsewhere (NVE): Intermediate Uveitis and Pars Planitis
Pars planitis — the most common form of intermediate uveitis — is an important cause of peripheral retinal and vitreous base neovascularization. Characteristic early findings include inferior peripheral venous dilatation and phlebitis, with progressive venular sheathing and obliteration. The resulting peripheral ischaemia, combined with the local inflammatory milieu, drives the release of vasogenic factors — including VEGF — that promote neovascularization of the peripheral retina and vitreous base.
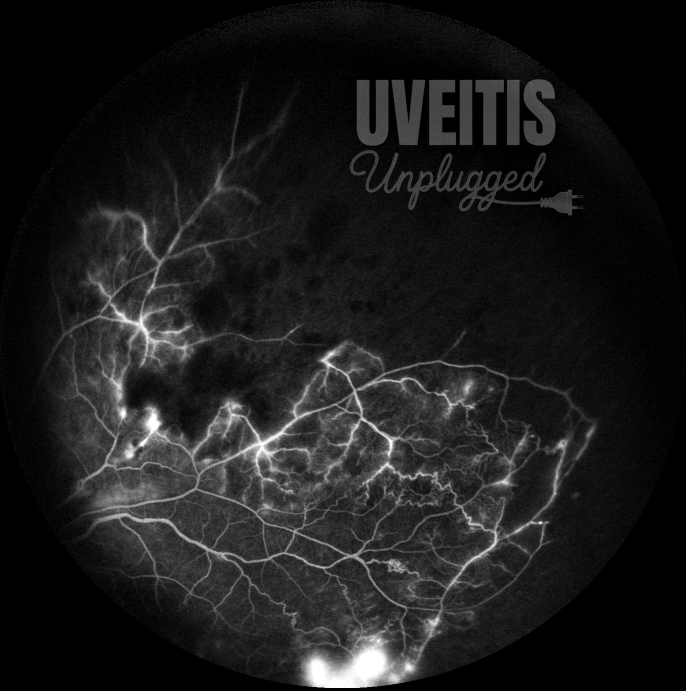
Peripheral neovascularization in pars planitis is common but often subtle, and may be missed on routine indirect ophthalmoscopy. Wide-field fluorescein angiography is essential for its detection. Children with intermediate uveitis are at higher risk of vitreous haemorrhage than adults (Lauer et al.). Left untreated, recurrent haemorrhage and tractional or rhegmatogenous retinal detachment may develop from progressive vitreoretinal contraction of the fibroglial pars plana membrane.
Staging of Peripheral Neovascularization in Pars Planitis
|
Stage |
Features |
|
1 |
Classic snowbank with active exudates and peripheral vascular sheathing. |
|
2 |
First evidence of neovascularization — dilated new vessels arising from the pars plana; dilatation of pre-existing terminal retinal vessels posterior to the ora serrata. |
|
3 |
Increased telangiectatic vessels and neovascular tissue overlying the snowbank; elevated angioma-like lesion formation. |
|
4 |
Secondary retinal detachment with haemorrhage and exudation in the subretinal space, intraretinal tissue, and vitreous — a direct consequence of peripheral neovascularization. |
A rare Coats' disease-like response has been reported in pars planitis (Suh et al.), attributed to VEGF-mediated vascular hyperpermeability — augmented by both inflammatory mediators and active neovascularization. This same mechanism underlies cystoid macular oedema, the leading cause of chronic visual morbidity in intermediate uveitis.
Key Points: NVE in Intermediate Uveitis
• Peripheral neovascularization is common but subtle — wide-field fluorescein angiography is essential and should not be deferred.
• Children with intermediate uveitis are at higher risk of vitreous haemorrhage than adults — a lower threshold for treatment is warranted.
• Untreated NVE progresses to tractional and rhegmatogenous retinal detachment from vitreoretinal fibrous contraction.
• A Coats'-like exudative response can occur — VEGF-driven hyperpermeability from inflammation and neovascularization combined.
• Cryotherapy to the snowbank ablates the angiogenic stimulus and promotes regression of peripheral neovascularization.