Periocular Corticosteroid
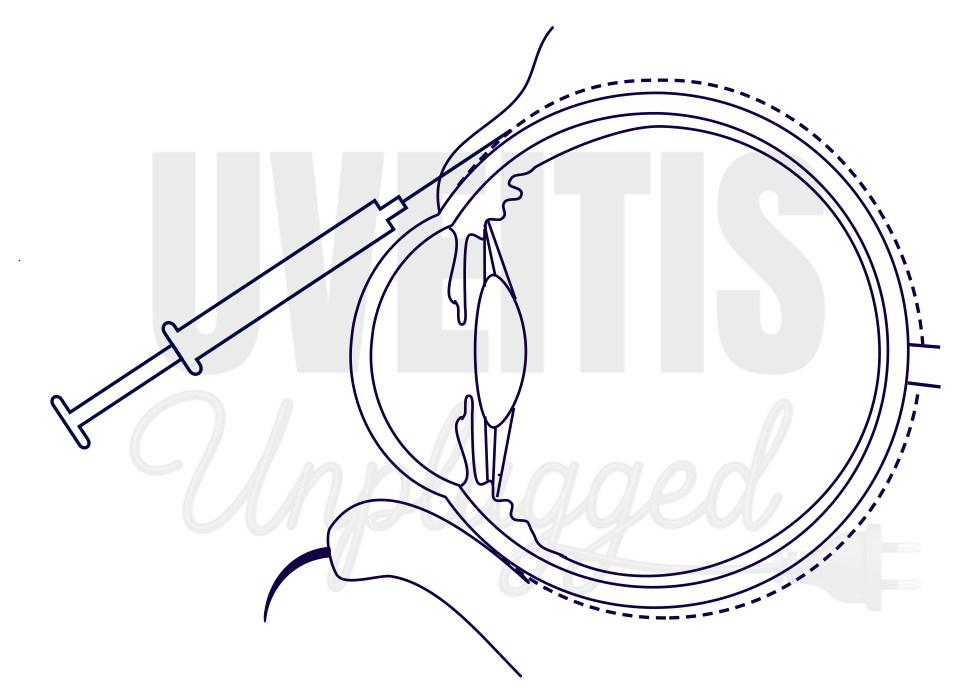
Periocular literally means “around the eye.” In clinical practice, periocular delivery refers to administering medication into the tissues surrounding the globe to achieve high local drug levels within the eye while minimizing systemic exposure . Periocular corticosteroid injections allow a relatively high concentration of steroid to be placed adjacent to the eye, promoting more consistent intraocular penetration and reducing systemic side effects. When delivered into the sub-Tenon’s space, the drug is retained within a closed compartment and released slowly, maintaining sustained local tissue levels over time. Periocular corticosteroids can be administered through several routes, including:
- Subconjunctival injection – into the subconjunctival space
- Sub-Tenon injection – beneath Tenon’s capsule (anterior or posterior)
- Orbital floor approach – transcutaneous injection through the temporal lower eyelid
- Retrobulbar or peribulbar injection – deeper orbital injections around the globe
This targeted approach provides effective local therapy with reduced systemic adverse effects.

Advantages and disadvantages of Periocular Steroid:
|
Advantages |
Disadvantages |
|
1. More amount of the drug is delivered to the eye |
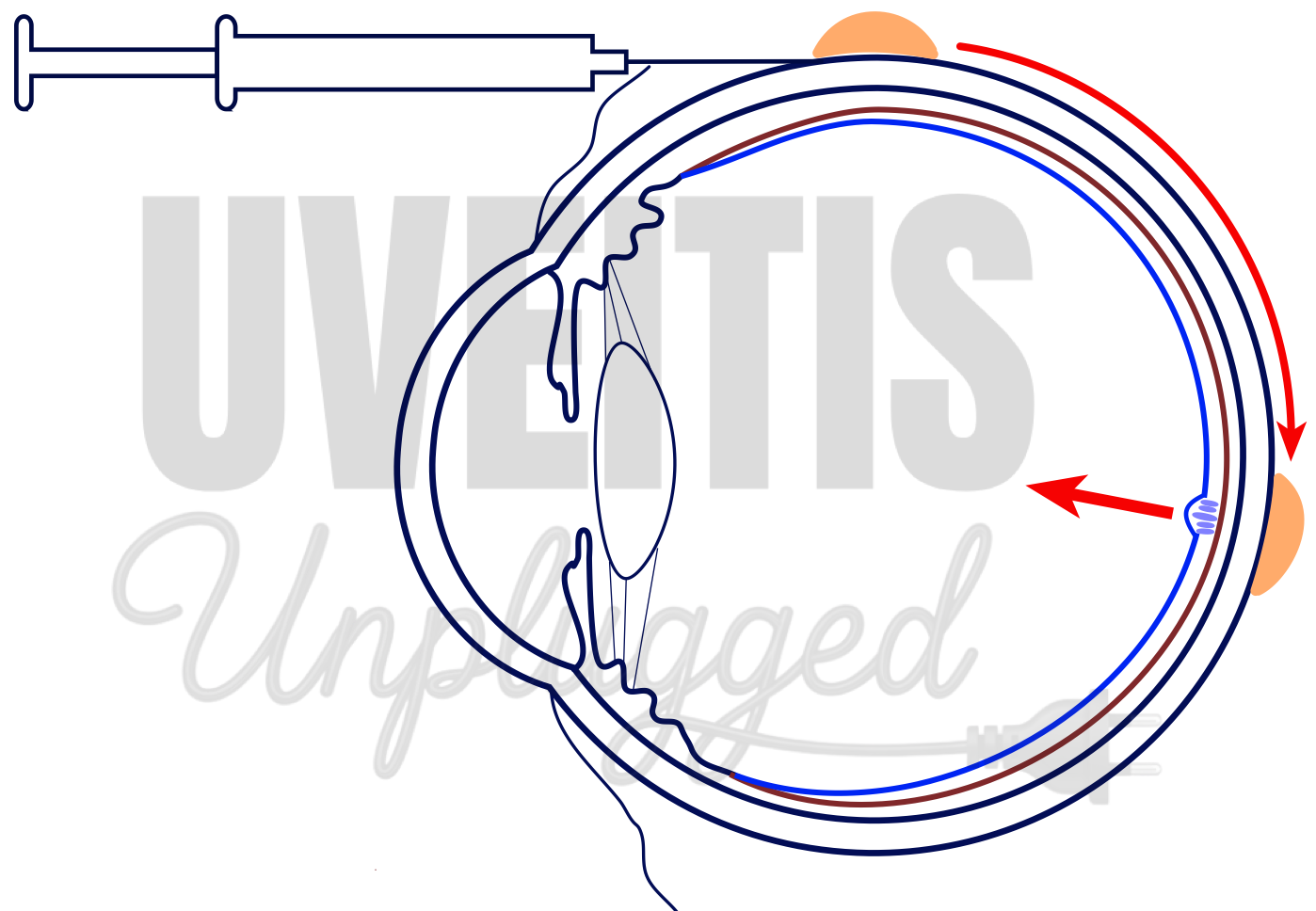
1. Majority of the drug injected in sub-tenon space is washed away by the highly vascular choroidal circulation before reaching the desired site |
|
2. More amount of the drug reaches posterior segment |
2. Less amount of drug reaches posterior segment when compared with intravitreal route |
|
3. Relatively easy to inject. Can be injected in out-patient department |
3. Chances of inadvertent perforation of the globe, ptosis can occur |
|
4. Chances of systemic side-effects is almost nil |
4. Complications like glaucoma, cataract formation are common |
|
5. Not dependent on patient’s compliance |
5. Once injected, removal can be difficult |
Various routes of periocular steroid injection has its own advantages and disadvantages, and one must be aware of it before deciding it only on the basis of their ease of comofrt on the technique.
|
Periocular corticosteroid injections |
Technique |
Primarily Used for |
Disadvantages |
|
Subconjunctival Injection |
Injecting the drug into subconjunctival space |
Useful for treatment of anterior segment inflammation |
Higher risk of raised IOP |
|
Anterior Subtenon Injection |
Injecting the drug beneath Tenon’s capsule either anteriorly or posteriorly |
Useful for treatment of anterior segment inflammation |
Higher risk of raised IOP |
|
Posterior Subtenon Injection |
Injecting the drug beneath Tenon’s capsule either anteriorly or posteriorly |
More effective for posterior segment inflammation particularly for macular edema |
Higher risk of inadvertent globe perforation and ptosis, Depot is difficult to remove, Post injection fibrosis can affect eventual surgery |
|
Orbital floor injection |
Transcutaneous injection through the temporal third of the lower eyelid to place the drug alongside the globe |
Idiopathic orbital inflammation Less chances of globe perforation, compared to other technique |
Not effective for macular edema. Leads to variable and significantly lower intraocular concentrations |
|
Retrobulbar Injection |
More effective for posterior segment inflammation particularly for macular edema |
High chances of damage to optic nerve |
Terms such as peribulbar, periocular, and parabulbar are often used interchangeably, but in practice they frequently refer to posterior sub-Tenon (PST) injection, the most commonly used periocular steroid technique. The superotemporal posterior sub-Tenon approach is preferred because it allows more accurate placement of the steroid depot close to the sclera behind the macula, while reducing the risk of globe perforation.
Indications
Periocular steroid injections are particularly useful in unilateral disease and in situations where systemic steroids should be avoided. Common indications include:
- Severe anterior segment inflammation
- Pars planitis
- Uveitic cystoid macular edema
- Preoperative or perioperative control of inflammation in uveitic eyes
- Posterior segment inflammation when systemic therapy is undesirable
Pharmacokinetics
- Triamcinolone acetonide is a long-acting synthetic steroid with low water solubility, resulting in a depot effect that may last up to 12 weeks.
- Detectable steroid levels have been reported months after injection.
- Exact dose equivalence between systemic and periocular steroids is unclear; a 40 mg PST injection has been suggested to approximate moderate oral dosing.
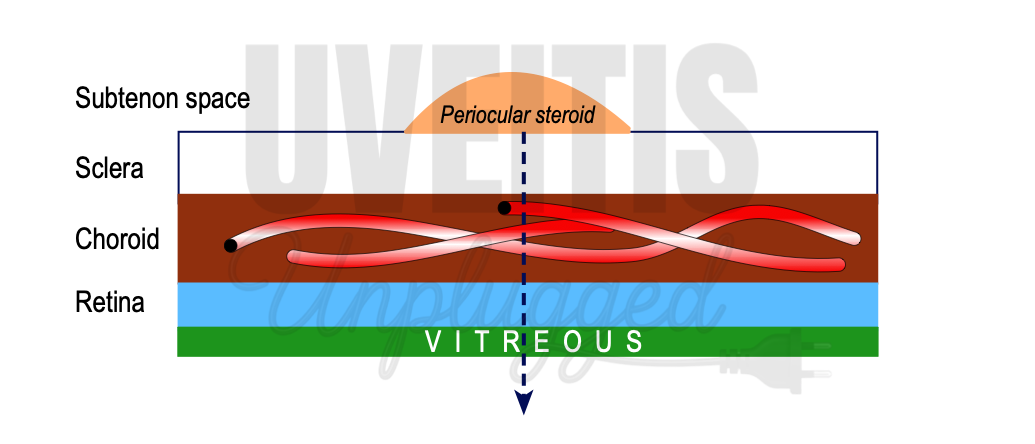
- After sub-Tenon injection, the drug must diffuse across the sclera, choroid, and retinal pigment epithelium to reach the retina.
- Methylprednisolone acetate (40 mg/mL) has been studied as an alternative to triamcinolone for orbital floor/periocular injections (OFCI/PSTI) in pediatric and adult uveitis, offering a shorter-acting profile but inferior depot effect.
- Vitreous concentrations with posterior sub-Tenon (PST) triamcinolone injections are significantly lower than with intravitreal injections (e.g., 1.22 ± 0.24 μg/ml vs. <0.001 μg/ml), as the drug must trans-sclerally diffuse across the sclera and choroid before reaching the vitreous, undergoing partial washout by the choroidal vasculature while traversing the choroid.
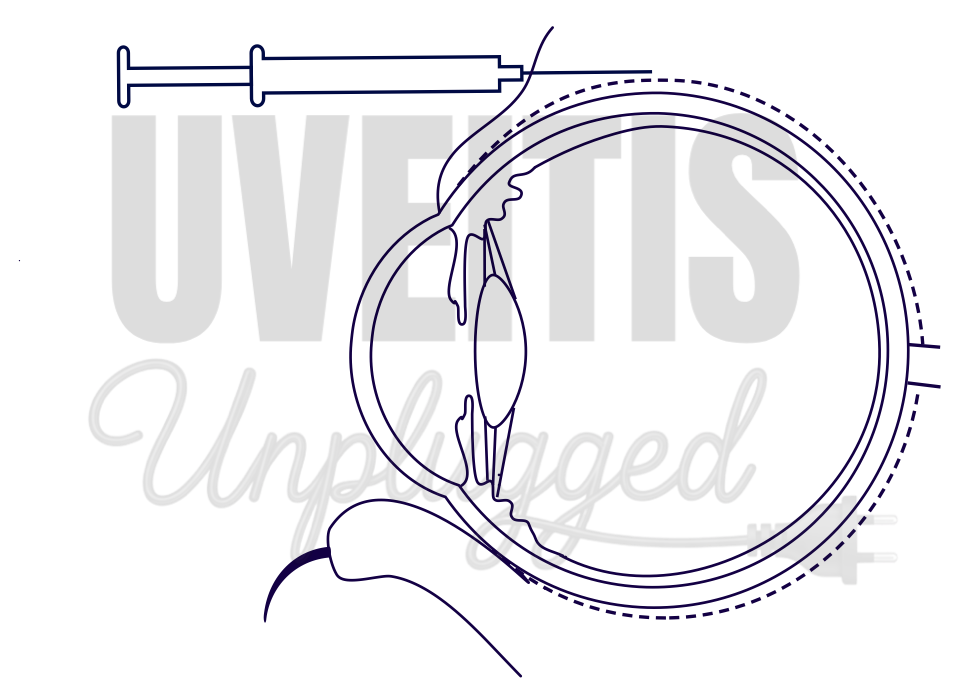
Technique: Posterior Sub-Tenon Injection (Smith & Nozik Method)
The Smith and Nozik technique is widely practiced.
- The patient lies supine.
- Topical anesthesia is applied.
- The superotemporal quadrant is selected.
- The patient looks inferonasally.
- A needle is introduced through the conjunctiva and Tenon’s capsule, keeping close contact with the sclera.
- The needle is advanced posteriorly toward the macular region.
- Once properly positioned, 0.5–1 mL of triamcinolone acetonide (40 mg/mL) is injected slowly using a 26-gauge needle.
The superotemporal route provides better retromacular drug placement compared to inferior approaches. Although inferotemporal injection may allow easier removal of the depot, it does not reliably achieve retromacular delivery.
Sub-Tenon injection requires precision, as the needle must remain close to the sclera, which increases the risk of perforation. Careful post-injection examination is essential.
Complications
Most are mild and self-limiting, but serious events can occur.
Common:
- Pain at injection site
- Eyelid swelling or pseudoptosis
- Subconjunctival hemorrhage
Less common but significant:
- Accidental globe perforation
- Cataract formation
- Ptosis
- Orbital fat atrophy
- Strabismus
- Conjunctival necrosis
Rare but serious:
- Central retinal artery occlusion
- Intra-arterial injection or choroidal/retinal penetration
Increased intraocular pressure (IOP):
-
More likely in patients known to be steroid responders.
