Managing Cataract in Children with Uveitis : A Challenge
Brief write-up for my ISU 2026 talk on pediatric uveitic cataract

Cataract remains the most frequent vision-threatening complication of childhood uveitis. In the developing visual system, lens opacification is not merely a reversible optical obstacle; prolonged visual deprivation during the amblyogenic period can result in irreversible cortical visual impairment. Consequently, every management decision—from inflammation control and corticosteroid exposure to surgical timing and intraocular lens (IOL) implantation—has profound implications for long-term visual outcomes.
The burden of cataract in paediatric uveitis is substantial. In the largest population-based analysis to date, the international TriNetX cohort comprising more than 22,000 propensity-matched children demonstrated a 17-fold increased risk of cataract in patients with uveitis over a 20-year follow-up (HR 17.17, 95% CI 12.90–22.80), with the excess risk consistently observed across age groups, sex, and ethnicities (1). Complementing these population-level data, tertiary referral series report cataract prevalence ranging from 18% to 44%, with the highest rates observed in chronic anterior uveitis, panuveitis, and late-presenting disease (2). Importantly, this variability largely reflects differences in the duration and adequacy of inflammatory control, underscoring that cataract development is not simply a consequence of uveitis itself, but of cumulative inflammatory burden and its treatment. You can browse the Comparison of Cataract Prevalence across 41 Published Case Series by clicking this link
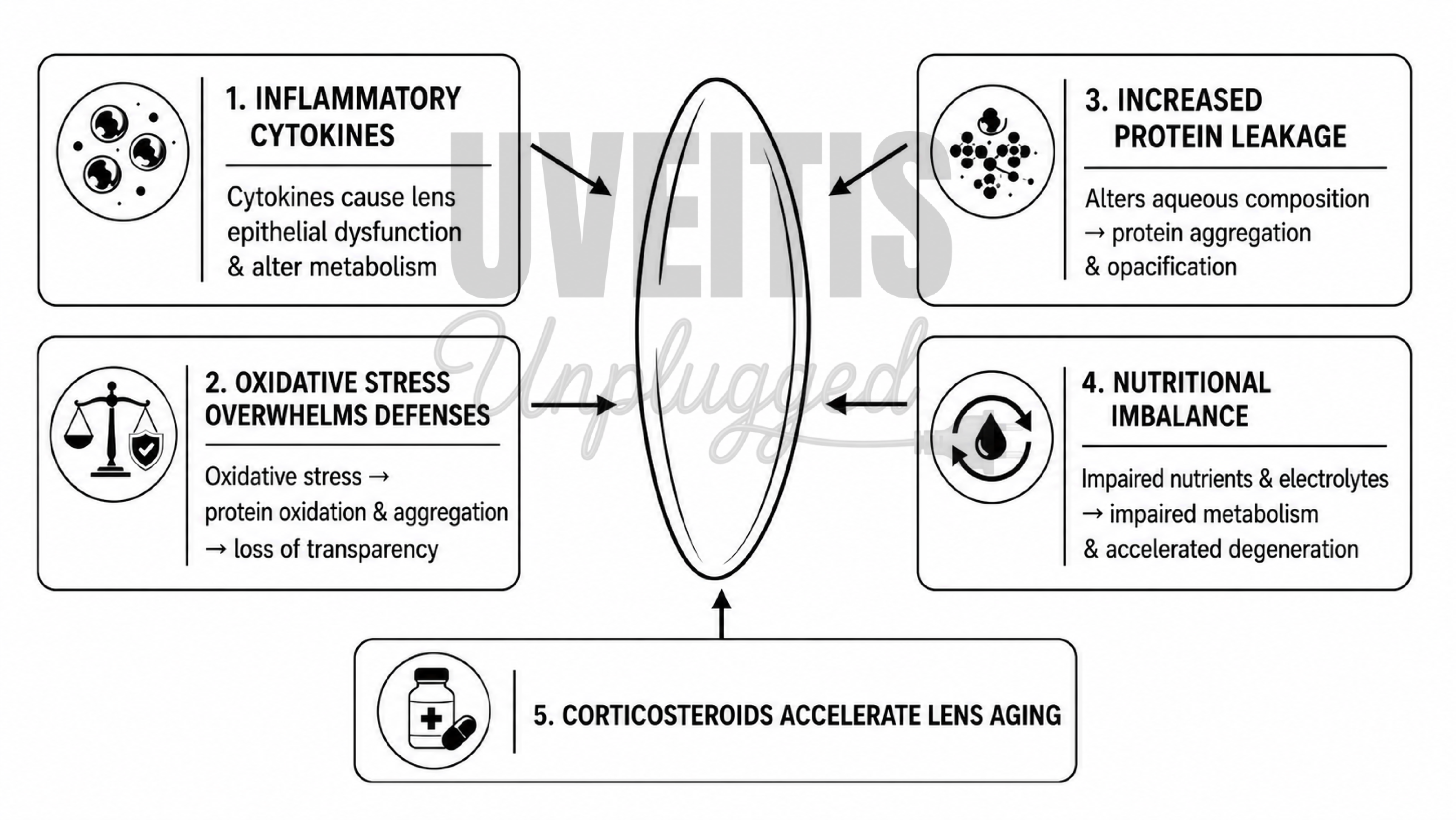
The uveitic lens is damaged from two directions at once. Chronic inflammation breaks down the blood–aqueous barrier, and cytokines such as IL-6 and IL-8, together with reactive oxygen species, act directly on lens epithelial cells — driving abnormal proliferation, migration and a self-amplifying fibrotic loop. This is why inflammation can cloud the lens even before heavy steroid exposure. On top of this, corticosteroids independently produce the classic posterior subcapsular cataract through altered lens-epithelial gene expression and aberrant cell migration. The lens, in short, pays twice — once for the disease and once for its treatment.
What the Risk-Factor Data Show
In a multicentre cohort of 247 eyes, the strongest independent driver of cataract was not any drug but inflammatory burden — flares per year (HR 3.06), followed by cystoid macular oedema (HR 2.87) and posterior synechiae at presentation (HR 2.85). Systemic and topical steroids were not significant once inflammation was accounted for; the only steroid route that was independently cataractogenic was local peri-ocular injection (HR 2.37) (2). One morphology deserves special respect: a nuclear cataract at baseline independently predicts a recalcitrant, treatment-resistant course of JIA-associated uveitis, and should prompt earlier escalation of immunosuppression (3).
The Steroid Nuance: Route and Dose, Not Systemic Use Itself
The association between corticosteroid therapy and cataract formation is determined primarily by the route, cumulative exposure, and treatment intensity rather than steroid use per se. In the Johns Hopkins JIA-associated uveitis cohort, topical corticosteroids demonstrated a clear dose-dependent relationship with cataract risk. Eyes receiving ≤3 drops/day had an 87% lower incidence of cataract than those receiving >3 drops/day (0.01 vs. 0.16 cataracts per eye-year), while maintenance therapy with ≤2 drops/day was associated with essentially no measurable excess risk (4). In contrast, periocular corticosteroid depot injections have consistently emerged as an independent risk factor for cataract development (2). Short-term systemic corticosteroids, when used judiciously to induce perioperative or disease quiescence, are unlikely to be the principal driver of lens opacification.
|
Route |
Cataract Risk |
Reference |
|
Topical ≤2 drops/day |
No measurable excess risk (0 eye-year; 95% CI upper 0.03) |
Thorne |
|
Topical ≤3 drops/day |
Very low risk (0.01/eye-year); 87% lower risk than >3 drops/day (RR 0.13) |
Thorne |
|
Topical >3 drops/day |
High risk (0.16/eye-year, P=0.0006) |
Thorne |
|
Periocular steroid injection |
HR 2.37 (1.18–4.75) |
Blum-Hareuveni 2017 |
|
Periocular steroid (JIA-U) |
Earlier cataract surgery HR 3.23 |
Sijssens 2007 |
|
Topical steroid use (overall) |
HR 29.5 vs 16.5 in non-users |
Hsu 2024 |
|
Systemic corticosteroids |
Not an independent risk factor after adjusting for inflammation |
Blum-Hareuveni 2017 |
These findings reinforce a key therapeutic principle: adequate suppression of intraocular inflammation should take precedence over concerns regarding brief systemic corticosteroid exposure, while long-term topical corticosteroid therapy should be minimized to the lowest effective maintenance dose. In children, the major limitation of prolonged systemic corticosteroid therapy lies less in cataractogenesis than in its well-recognized systemic toxicities, including impaired linear growth, reduced bone mineral density, and metabolic adverse effects. Nevertheless, clinicians must remain vigilant for steroid-induced ocular hypertension and secondary glaucoma, particularly in younger children, who are more susceptible to a pronounced steroid response.
Prevention: The Biologic Era Has Redefined Outcomes
The greatest opportunity to prevent cataract lies in early, effective, steroid-sparing immunomodulation. Over the past two decades, the introduction of conventional and biologic DMARDs has fundamentally altered the natural history of childhood uveitis. In a longitudinal Italian cohort, the transition from systemic corticosteroid-based therapy to methotrexate and biologics (principally adalimumab and infliximab) was associated with significantly fewer recurrences and a lower incidence of cataract, posterior synechiae, band keratopathy, and ocular hypertension compared with the pre-biologic era (5). The highest level of evidence comes from the SYCAMORE randomized controlled trial, in which the addition of adalimumab to stable methotrexate therapy reduced the risk of treatment failure by 75% (HR 0.25; 95% CI 0.12–0.49), albeit with an increased frequency of adverse events (6). The implication is straightforward: sustained inflammatory control reduces recurrent tissue injury, thereby preventing cataract formation. Early involvement of pediatric rheumatologists and seamless transition to adult care should therefore be viewed as integral components of long-term disease modification.
Timing of Surgery: Balancing Inflammatory Control Against Amblyopia
Preoperative inflammatory quiescence remains the single most important predictor of surgical success. Most contemporary series advocate at least three months of inactive inflammation before cataract surgery. In a Finnish cohort with 5–10 years of follow-up, active uveitis during the 3 and 12 months preceding surgery independently predicted poorer long-term visual acuity (7). However, prolonged surgical delay is not without consequence. In visually immature children, dense cataract produces irreversible deprivation amblyopia if left untreated. The objective, therefore, is not simply to postpone surgery, but to achieve rapid and sustained disease control, followed by intervention within the amblyogenic window. Interestingly, removal of the chronically inflamed lens may itself reduce ocular inflammatory activity; one series demonstrated a reduction in flare frequency from 3.7 to 1.6 episodes per eye-year following cataract extraction (3).
Disease Phenotype Determines Surgical Risk
Surgical prognosis varies substantially according to the underlying uveitic entity. Fuchs uveitis syndrome generally demonstrates favorable outcomes following phacoemulsification with primary IOL implantation, whereas JIA-associated chronic anterior uveitis remains the highest-risk phenotype, characterized by a greater incidence of postoperative fibrin formation, cyclitic membranes, hypotony, and recurrent inflammation. Long-term surveillance is equally important, as progressive zonular insufficiency may culminate in late in-the-bag IOL dislocation, occurring a mean of approximately seven years after apparently uncomplicated surgery (8). Surgical planning should therefore be individualized according to disease phenotype rather than applying a uniform strategy to all forms of pediatric uveitis.
Primary IOL Implantation: From Contraindication to Careful Selection
The traditional view that primary IOL implantation is contraindicated in pediatric uveitis, particularly JIA-associated disease, has evolved considerably. Earlier concerns that an IOL would perpetuate chronic inflammation, membrane formation, and phthisis have not been substantiated in carefully selected eyes receiving modern immunosuppressive therapy. Nemet and colleagues demonstrated that primary IOL implantation, including foldable acrylic lenses, was well tolerated in both JIA and non-JIA uveitis when inflammation was aggressively controlled, concluding that uveitis should no longer be regarded as an absolute contraindication to IOL implantation (9). Similarly, a French series with a median follow-up of six years (maximum 19 years) reported corrected visual acuity of ≤0.3 logMAR in all eyes undergoing in-the-bag IOL implantation after at least three months of quiescence, concluding that controlled uveitis is compatible with excellent long-term outcomes (10). Comparable long-term results have also been reported in Finnish children with well-controlled JIA-associated uveitis (7).
|
Age group (uveitic child) |
Surgical consideration |
Evidence / rationale |
|
Infants / very young (<2 yr) |
Uveitic cataract rare here; if present, favour aphakia + contact lens; avoid primary IOL |
High glaucoma/inflammatory-membrane risk; refractive instability¹ ² ⁴ |
|
Young child (~2–6 yr) |
Individualise; aphakia often preferred; primary IOL only if inflammation is well controlled and follow-up assured |
IOL less well tolerated in young inflamed eyes; amblyopia must be managed¹¹ |
|
Older child (≥6–7 yr) |
Primary IOL implantation gives good results in well-selected, quiescent eyes |
Terrada (median 9.5 yr) and others: uveitis is not a formal contraindication with full inflammation control⁶ ⁷ ⁸ |
|
Any age with active/poorly controlled uveitis |
Defer surgery until sustained quiescence (≥3 months) |
Pre-operative quiescence is the strongest predictor of good outcome⁶ ⁹ |
Evidence synthesized across comparative studies further supports this paradigm shift. A systematic review and meta-analysis of ten studies demonstrated superior visual acuity in pseudophakic compared with aphakic eyes at both one and five years, without an increase in overall postoperative complications, apart from a higher incidence of visual-axis opacification and a lower incidence of hypotony in pseudophakic eyes (11). Likewise, Sijssens et al. reported that primary IOL implantation did not increase the risks of ocular hypertension, secondary glaucoma, cystoid macular edema, or optic disc swelling, while providing superior visual rehabilitation, although these children also received more intensive methotrexate therapy (12).
When Aphakia Remains the Preferred Strategy
Primary aphakia remains appropriate in selected situations. Eyes with persistent inflammation, disease quiescence of less than three months, very young age, posterior segment involvement, cyclitic membranes, hypotony, or uncertain long-term compliance are generally better managed with pars plana lensectomy combined with vitrectomy. Vitrectomy removes the vitreous scaffold that supports persistent inflammatory membranes and cyclitic bands, although optical rehabilitation subsequently relies on contact lenses or aphakic spectacles until secondary IOL implantation becomes feasible. Current practice patterns continue to reflect differing philosophies; pediatric ophthalmologists are significantly more likely than uveitis specialists to avoid primary IOL implantation in chronic JIA-associated uveitis, pars planitis, or recurrent anterior uveitis despite adequate inflammatory control (13). Contemporary evidence therefore supports patient selection rather than dogma, reserving primary IOL implantation for older children with well-controlled disease, while favoring aphakia in younger patients or those with persistent inflammatory risk.
|
Outcome |
Phaco–IOL |
Lensectomy–Vitrectomy (Aphakia) |
|
Visual acuity |
↑ Better visual outcomes* |
Lower* |
|
Hypotony |
↓ Less frequent* |
More frequent* |
|
Visual axis opacification |
↑ More common |
↓ Less common |
|
Postoperative inflammation |
Slightly higher |
Trend toward lower |
|
Glaucoma / Resurgery |
Similar |
Similar |
Perioperative Management and Postoperative Challenges
Cataract surgery in pediatric uveitis remains technically demanding. Surgeons should anticipate posterior synechiae, poor pupillary dilation, capsular fibrosis, and a vigorous postoperative fibrin response. Surgical adjuncts—including trypan blue staining, viscodissection of synechiae, iris hooks or Malyugin rings, and primary posterior capsulotomy with anterior vitrectomy in younger children—are frequently required to optimize surgical outcomes. Intensive perioperative immunosuppression, combining systemic and topical corticosteroids with uninterrupted DMARD or biologic therapy, has become standard practice.
Despite meticulous perioperative management, postoperative complications remain common, occurring in approximately 40–75% of eyes. Visual-axis opacification remains the most frequent complication, followed by secondary glaucoma, cystoid macular edema, and hypotony, the latter representing the principal threat to long-term globe survival. Nevertheless, contemporary series consistently report visual improvement in approximately 80% of operated eyes. Clinicians should remain particularly vigilant when postoperative macular edema develops, as distinguishing Irvine–Gass syndrome from recurrent uveitis may be challenging. Furthermore, any postoperative inflammation that appears disproportionate or progressively worsening should be managed as infectious endophthalmitis until proven otherwise, particularly in children, whose inflammatory responses are often exaggerated and whose symptom reporting may be unreliable.
Pearls for Managing Cataract in Children with Uveitis
- Wait for quiet: do not operate until the eye has been inflammation-free for at least 3 months; escalate immunosuppression pre-operatively rather than rushing to theatre.
- Respect the nuclear cataract: its presence flags a recalcitrant uveitis course — step up systemic therapy early.
- Load steroids peri-operatively: combine oral, topical and often intracameral/intravitreal steroid, and continue systemic immunomodulation through surgery.
- Keep maintenance drops low: aim for ≤3 (ideally ≤2) topical steroid drops/day; frequent drops and peri-ocular depot injections drive cataract.
- Assume a difficult pupil: keep iris hooks, a Malyugin ring and trypan blue on the trolley for the bound-down, poorly dilating pupil.
- Follow up for life: uveitic eyes develop late in-bag IOL dislocation years after surgery — do not discharge them.
